> For the complete documentation index, see [llms.txt](https://curriculum.covidstudentresponse.org/llms.txt). Markdown versions of documentation pages are available by appending `.md` to page URLs; this page is available as [Markdown](https://curriculum.covidstudentresponse.org/module-6-training-for-clinical-roles/mechanical-ventilation-the-basics.md).
# Mechanical Ventilation: The Basics
## Introduction
Patients with severe SARS-CoV-2 may require mechanical ventilation, currently in an intensive care unit (ICU). However, they may require ventilation in non-ICU settings as well. Sole management of a mechanical ventilator may not currently be a medical student’s responsibility, given recent changes regarding graduating 4th year medical students into early interns, this section is included to familiarize medical students with the terminology of mechanical ventilation. The hope is to educate medical students on the basics of mechanical ventilation in preparation for their future roles as physicians. As this section provides only a basic introduction, please refer to the linked resources for details.
Acute respiratory distress syndrome (ARDS) is a recognized complication of severe COVID-19 infection ([Zhou et al. Lancet 2020](https://www.thelancet.com/journals/lancet/article/PIIS0140-6736\(20\)30566-3/fulltext); [Wu et al. JAMA Intern Med. 2020](https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2763184)). In ARDS, a dysregulated immune response leads to pulmonary edema, making oxygenation difficult ([Mora Carpio and Mora StatPearls](https://www.ncbi.nlm.nih.gov/books/NBK448186/); [AMBOSS](https://www.amboss.com/us/knowledge/Acute_respiratory_distress_syndrome)). Mechanical ventilation is usually required to maintain adequate arterial oxygen levels ([AMBOSS](https://www.amboss.com/us/knowledge/Acute_respiratory_distress_syndrome)). In the sections below, look out for references to mechanical ventilator management in ARDS.
## Review of Essential Concepts and Definitions
### The three parts of the respiratory system
The respiratory system can be conceptually separated into three parts: the **controller**, the ventilatory **pump**, and the gas **exchanger** ([Schwartzstein and Parker, Respiratory Physiology: A Clinical Approach](https://www.amazon.com/Respiratory-Physiology-Clinical-Approach-Integrated/dp/0781757487/)). The controller regulates the respiratory rate (RR) and the depth (tidal volume) of breathing. The ventilatory pump includes the neuromuscular apparatus for breathing as well as the airways, and serves to move air from the mouth to the alveoli and back. The gas exchanger describes the alveolar-capillary interface, and allows for the diffusion of oxygen into the blood and carbon dioxide out of the blood. Together, the three parts of the respiratory system perform the two main functions of oxygenation and mechanical ventilation ([UC Denver](http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/intmed/imrp/CURRICULUM/Documents/Mechanical%20ventilation%20review.pdf)).
* Oxygenation: getting O2 into the body
* Ventilation: getting CO2 out of the body
### Who requires mechanical ventilation?
There are several indications for mechanical ventilation ([Merck Manuals](https://www.merckmanuals.com/professional/critical-care-medicine/respiratory-failure-and-mechanical-ventilation/overview-of-mechanical-ventilation)). In general, patients who cannot perform adequate oxygenation or ventilation on their own (respiratory failure from conditions such as ARDS, pneumonia, pulmonary edema, COPD, asthma), as well as patients who cannot maintain a patent airway, should be considered for mechanical ventilation ([Lippincott](https://www.nursingcenter.com/getattachment/Clinical-Resources/nursing-pocket-cards/Mechanical-Ventilation-Settings-and-Basic-Modes/Mechanical-Ventilation-Settings-and-Basic-Modes-Tip-Card_January-2019.pdf.aspx); [Merck Manuals](https://www.merckmanuals.com/professional/critical-care-medicine/respiratory-failure-and-mechanical-ventilation/overview-of-mechanical-ventilation)). Ventilatory assistance can be provided using either a non-invasive route (e.g. CPAP, NIPPV) or an invasive route requiring endotracheal intubation (mechanical ventilation) depending on the clinical situation ([Merck Manuals](https://www.merckmanuals.com/professional/critical-care-medicine/respiratory-failure-and-mechanical-ventilation/overview-of-mechanical-ventilation)).
### Oxygenation and ventilation in a mechanically ventilated patient
Here’s how a mechanical ventilator accomplishes these two functions for a patient ([Mora Carpio and Mora, StatPearls](https://www.ncbi.nlm.nih.gov/books/NBK448186/)):
* **Oxygenation:** controlled by adjusting the fraction of inspired oxygen (FiO2) and the positive end-expiratory pressure (PEEP). Oxygenation can be conveniently measured by pulse oximetry (SpO2).
* **FiO2:** the fraction of air entering the airway of a patient that is made up of oxygen. This can be anywhere between 21% (ambient air) and 100%. Increasing the FiO2 can increase the PaO2, depending on the patient’s clinical circumstances and pathophysiology.
* **PEEP:** air pressure remaining in the airways at the end of expiration. In mechanically ventilated patients, PEEP is provided by the mechanical ventilator and is a positive pressure that is greater than the atmospheric pressure. Increasing the PEEP may increase PaO2, depending on the patient’s clinical status and pathophysiology.
* **Ventilation:** controlled by adjusting the minute ventilation.
* **Minute ventilation:** the volume of air moved into and out of the lungs per unit time, measured in L/min. Minute ventilation = RR x VT.
* **Tidal volume (VT):** volume of air moved into and out of the lungs in one breath.
### Pressure and compliance in a mechanically ventilated patient
When mechanically ventilating a patient, there are two pressure parameters that are important to keep in mind ([Mora Carpio and Mora, StatPearls](https://www.ncbi.nlm.nih.gov/books/NBK448186/); [UC Denver](http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/intmed/imrp/CURRICULUM/Documents/Mechanical%20ventilation%20review.pdf)):
* **Peak pressure:** the maximum pressure created by forcing the programmed tidal volume through a patient’s airways during inspiration. This parameter reflects airway resistance.
* **Plateau pressure:** equilibrium pressure in the respiratory system at the end of inspiration. This parameter reflects the compliance of the respiratory system (chest wall and lungs). You can measure the plateau pressure by conducting an inspiratory hold, which lets the pressure in the respiratory system equilibrate at the end of inspiration, such that the lower pressures in the alveoli and respiratory bronchioles (in which are generated by the compliance of the respiratory system) equilibrate with the larger airway (in which the pressures measured during the inspiratory phase of mechanical ventilation are generated by airways resistance). This allows one to measure the pressure in the lower respiratory tree and approximate the respiratory system compliance. Plateau pressure should be kept under 30cm H2O; higher plateau pressure may indicate low compliance, may result in trauma to the lungs, [and have been shown to result in increased mortality for patients with ARDS.](https://www.nejm.org/doi/full/10.1056/NEJM200005043421801)
**Compliance** is a fundamental concept in respiratory physiology. Compliance is equal to the change in volume over the change in pressure (C = ΔV/ΔP) ([Mora Carpio and Mora, StatPearls](https://www.ncbi.nlm.nih.gov/books/NBK448186/)). Some conditions, such as ARDS, may cause a patient’s lungs to be less compliant (stiffer); this means that for a given tidal volume, there is a greater than normal change in pressure.
### Additional definitions
Please see this chart for additional definitions ([Lippincott Ventilator Guide](https://www.nursingcenter.com/getattachment/Clinical-Resources/nursing-pocket-cards/Mechanical-Ventilation-Settings-and-Basic-Modes/Mechanical-Ventilation-Settings-and-Basic-Modes-Tip-Card_January-2019.pdf.aspx)).
*Thought questions:*
Which mechanical ventilator measure might suggest a state of low compliance in a patient with ARDS?
You are taking care of a patient with ARDS on a mechanical ventilator. You draw an arterial blood gas (good job!) and you note that the PaO2 is worrisome. Which mechanical ventilator settings could you change to improve oxygenation?
## Fundamentals of Mechanical Ventilator Settings
The following information is sourced from [Merck Manuals](https://www.merckmanuals.com/professional/critical-care-medicine/respiratory-failure-and-mechanical-ventilation/overview-of-mechanical-ventilation) and [Mora Carpio and Mora, StatPearls](https://www.ncbi.nlm.nih.gov/books/NBK448186/).
Your first choice in operating a mechanical ventilator is to provide the patient with either a specified **volume** of air (volume control or volume-cycled ventilation) or a specified **pressure** of air (pressure control or pressure-cycled ventilation). Remember that pressure and volume have an inverse relationship. In volume control, when you set a volume and a respiratory rate, pressure will vary based on the patient’s respiratory system compliance. In pressure control, when you specify a pressure, volume will vary, based on the patient’s respiratory system compliance. In general, volume control is used more often than pressure control.
PEEP will be used in either pressure or volume control. PEEP is used to, essentially, stent open alveoli that might otherwise collapse at the end of expiration. More open alveoli can improve gas exchange, leading to better oxygenation. As discussed above, another way of improving oxygenation would be to increase the FiO2.
Another important decision point in mechanical ventilator settings involves the control of the **initiation** of a breath. Either the vent or the patient can initiate a breath. In other words, either the machine can automatically begin a breath by pushing air into the lungs, or the machine can wait until the patient starts to take a breath before pushing air into the lungs.
### Noninvasive Positive Pressure Ventilation
Noninvasive positive pressure ventilation (NIPPV) is provided through a facemask that fits snugly over the patient’s face. An endotracheal tube is not required. As a broad generalization, NIPPV is used to try to improve oxygenation and ventilation in patients who are not yet sick enough for endotracheal intubation. The two most common forms of NIPPV are:
* **Continuous positive airway pressure (CPAP)**: machine delivers a constant positive pressure through the airways throughout inspiration and expiration. The same pressure is delivered by the machine during inspiration and expiration.
* **Bi-level ventilation**: machine delivers a set pressure through the airways during inspiration and a different set pressure through the airways during expiration. In other words, different pressures can be specified in inspiration and expiration ([Merck Manuals](https://www.merckmanuals.com/professional/critical-care-medicine/respiratory-failure-and-mechanical-ventilation/overview-of-mechanical-ventilation)).
Current [WHO treatment guidelines](https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-\(ncov\)-infection-is-suspected) are equivocal as to whether NIPPV should be used in SARS-CoV-2, but they do cite a study suggesting that NIPPV was generally ineffective in patients with ARDS due to MERS infection ([Arabi et al., Ann Intern Med 2014](http://ncbi.nlm.nih.gov/pubmed/24474051)). Their guidelines state that NIPPV “should only be used in selected patients with hypoxemic respiratory failure.”
Informal guidance ([ICU one pager](https://www.onepagericu.com/)) has noted that CPAP and NIPPV should generally be avoided in patients with COVID-19, as these methods might potentially aerosolize virus particles.
### Modes of mechanical ventilation
Here are three common types of mechanical ventilator configuration, often referred to as “modes.” You might see the abbreviations listed on patient lists during rounds.
The following information is sourced from [Merck Manuals](https://www.merckmanuals.com/professional/critical-care-medicine/respiratory-failure-and-mechanical-ventilation/overview-of-mechanical-ventilation), [Mora Carpio and Mora, StatPearls](https://www.ncbi.nlm.nih.gov/books/NBK448186/), and [UC Denver](http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/intmed/imrp/CURRICULUM/Documents/Mechanical%20ventilation%20review.pdf) and [SOCCA ICU Residents’ Guide](https://www.umassmed.edu/globalassets/anesthesiology/files/resources/2016-resources/2014-socca-residents-guide.pdf).
#### AC (Assist control) = CMV = Continuous Mandatory Ventilation
* “Assist”: If the patient is at or above the set RR. When the patient tries to inspire, the mechanical ventilator pushes in air.
* “Control”: If the patient is below the set RR. The mechanical ventilator will deliver air at the set RR regardless of the patient’s efforts at inspiration.
* So the vent delivers air at or above a minimum RR, and all breaths are assisted.
#### Pressure support ventilation (PSV)
* Breaths triggered by the patient only (not set respiratory rate from the mechanical ventilator)
* Delivers a baseline PEEP, and an additional pressure of air above this PEEP during each patient-initiated inspiration
* Frequently used for weaning patients from the vent
There are many additional modes which are omitted here for brevity. Some are described in a handy chart in the [Lippincott Ventilator Guide](https://www.nursingcenter.com/getattachment/Clinical-Resources/nursing-pocket-cards/Mechanical-Ventilation-Settings-and-Basic-Modes/Mechanical-Ventilation-Settings-and-Basic-Modes-Tip-Card_January-2019.pdf.aspx).
### How do I set a mechanical ventilator? ([Merck Manuals](https://www.merckmanuals.com/professional/critical-care-medicine/respiratory-failure-and-mechanical-ventilation/overview-of-mechanical-ventilation))
1\) Mode: AC, PC, PSV, etc.
2\) Rate: Minimum breaths/minute (if indicated - not appropriate for PSV)
3\) Tidal Volume: always target 6cc per kilogram of ideal body weight (based on the patient's height, not their actual weight) for assist-control ventilation. This is not applicable for PSV.
4\) FiO2 = start at 100% and titrate down as you are able based on the patient’s SpO2
5\) PEEP = it is generally OK to start with 5 mmHg (but have a low threshold to increase up to 10-15mm Hg in hypoxemic patients)
Note that (1), (2), (3) are all related to CO2, whereas (4) and (5) refer primarily to O2.
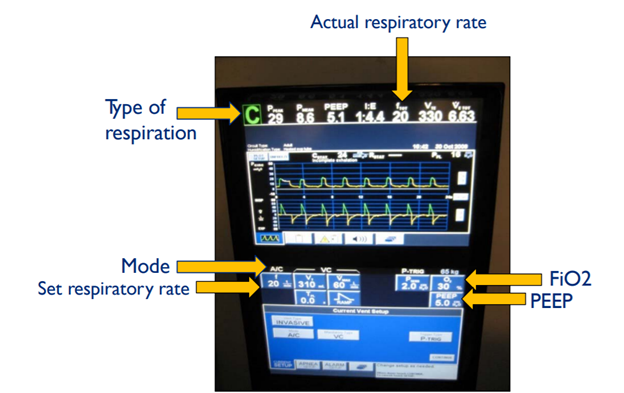
Sample Mechanical Ventilator Settings (Source: [Johns Hopkins Ventilator Guide](https://www.johnshopkinssolutions.com/wp-content/uploads/2017/10/4-Understanding-Mechanical-Ventilation.pdf))
### How is a mechanical ventilator used for ARDS?
Acute respiratory distress syndrome (ARDS) is a complication of many different pulmonary and systemic processes, including severe SARS-CoV-2 ([Zhou et al. Lancet 2020](https://www.thelancet.com/journals/lancet/article/PIIS0140-6736\(20\)30566-3/fulltext); [Wu et al. JAMA Intern Med. 2020](https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2763184)). In ARDS, an explosive pulmonary or systemic inflammatory response damages pulmonary vasculature, resulting in non-cardiogenic pulmonary edema that can trigger hypoxemic respiratory failure. Patients with ARDS often need ICU-level care and mechanical ventilation ([AMBOSS](https://www.amboss.com/us/knowledge/Acute_respiratory_distress_syndrome)).
In mechanical ventilation of ARDS patients, including patients with ARDS from COVID-19, the goal is to provide low tidal volumes and low inspiratory pressures. This approach, known as **lung-protective ventilation (LPV)**, can help avoid mechanical ventilator-associated lung injury ([AMBOSS](https://www.amboss.com/us/knowledge/Acute_respiratory_distress_syndrome); [ARDSnet](http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf); [WHO](https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-\(ncov\)-infection-is-suspected)).
**Inclusion Criteria for Mechanical Ventilator Use in ARDS (**[**ARDSnet**](http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf)**):**
Acute onset of
1. PaO2/FiO2 ≤300
2. Pulmonary edema (bilateral pulmonary infiltrates on CXR) not thought to be due to left-sided heart failure
3. Bilateral alveolar infiltrates on chest x-ray
**Mechanical Ventilation Protocol (**[**ARDSnet**](http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf)**):**
Mechanical Ventilator goals:
* Oxygenation: PaO2 55-80 mmHg or SpO2 88-95%
* Plateau pressure: ≤30 cm H2O
* pH: 7.30-7.45
* I:E ratio: inspiration ≤ expiration
**Weaning:** when patient improves and meets [criteria](http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf), conduct a daily **spontaneous breathing trial (SBT)**
* Assess the ability of the patient to breathe with minimal or no mechanical ventilator support
* If trial is unsuccessful, resume pre-weaning settings
For a quick guide to extubating a patient ([click here](https://twitter.com/nickmmark/status/1242574416166277121)).
For more detailed information on mechanical ventilator settings for ARDS ([click here](http://www.ardsnet.org/files/ventilator_protocol_2008-07.pdf)).
For quick ICU guidelines for COVID ([click here](https://www.onepagericu.com/)).
For more information on clinical trials regarding mechanical ventilation, refer to supplementary material in Module 1 ([click here](https://docs.google.com/document/d/1SsWujt6g1iNUAAPeOFjSP8YFaK_C48SSO_2iz0BcQi4/edit#bookmark=id.8ldb2jkztow5)).
*Thought question:*
* Why might a slight respiratory acidosis be tolerated in a patient with ARDS? In other words, if you are taking care of a patient with ARDS whose PaCO2 is above normal, why would you not increase the tidal volume to increase the minute ventilation?
## Simulator
For an opportunity to apply these concepts while interacting with a ventilator control panel, please work through this [Ventilator Simulator](https://www.openpediatrics.org/assets/simulator/ventilator-simulator) created by OpenPediatrics.