> For the complete documentation index, see [llms.txt](https://curriculum.covidstudentresponse.org/llms.txt). Markdown versions of documentation pages are available by appending `.md` to page URLs; this page is available as [Markdown](https://curriculum.covidstudentresponse.org/module-4-mental-health-in-the-time-of-covid-19/evolving-clinical-practices-in-mental-healthcare.md).
# Evolving Clinical Practices in Mental Healthcare
As we have shown throughout the module, many individuals are at risk for worsening mental health outcomes as a result of the pandemic. Given the existing [shortage](https://bhw.hrsa.gov/sites/default/files/bhw/nchwa/projections/state-level-estimates-report-2018.pdf) of mental healthcare providers in our country and the increasing demand, we can expect increasing strain on mental healthcare services in the future.
Here, we describe how the ways in clinicians support patients and provide clinical care may evolve as a consequence of the COVID-19 pandemic. How mental health care systems will continue to evolve over time is not possible to predict, but we can expect changes at all levels of psychiatric care and a move towards increased telehealth services. In addition, we can expect a significant rise in post-traumatic stress symptoms among our patients making trauma-informed approaches to clinical care essential.
## Escalation of Psychiatric Care and Mental Health Resources
Resources for mental health support are, at baseline, often confusing given different types of providers (ie., MDs, PhDs, PsyDs, social workers) and care settings (community organizations, peer groups, hospitals, clinics). In addition, gaps in mental healthcare insurance coverage and high out of pocket costs often limit patients from obtaining the care they need. As mental healthcare resources in our country become increasingly strained by the demand for services, it will come increasingly important to recognize and recommend clinically appropriate care for our patients. One model to think through this decision is a system of care approach, that has been previously utilized in many global health settings, shown below:
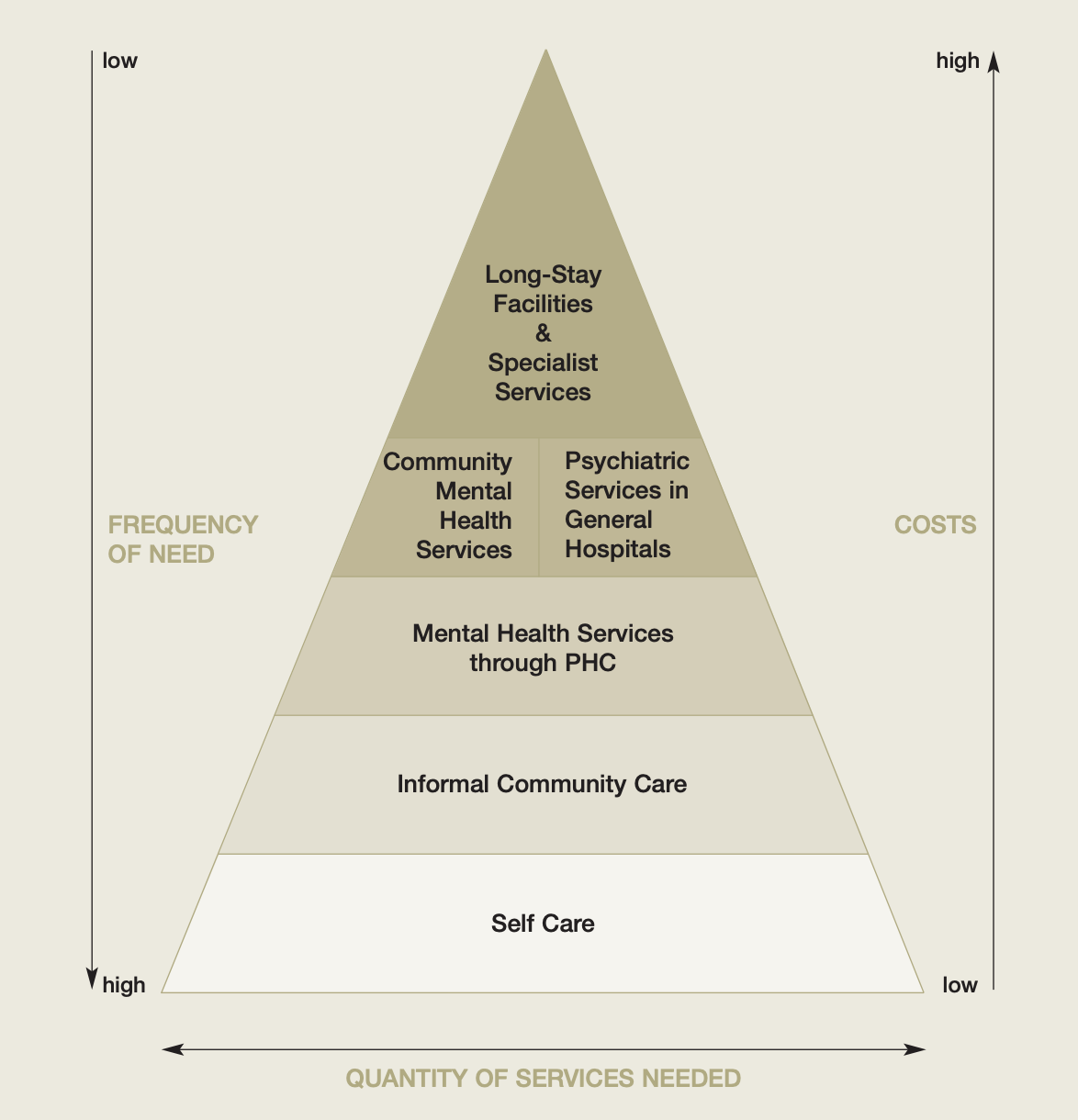
([“Organization of Services for Mental Health,” World Health Organization, 2003](https://www.who.int/mental_health/policy/services/4_organisation%20services_WEB_07.pdf?ua=1))
This model compares various options for psychiatric support based on cost and frequency of need. Here, lower cost resources, such as self care, should be used broadly by the population while higher cost ones such as psychiatric hospital services are used less frequently.
This framework helps us think through which level of care is appropriate for our patients. For example, Brian may benefit most from self-care techniques and connection to community resources. For Diane, on the other hand, these techniques may be insufficient. Patients may need to move up the pyramid to a more intensive system of care. Of note, this approach is not advocating for a rationing of care, as discussed in [Module 7](https://curriculum.covidstudentresponse.org/module-6-medical-ethics-in-relation-to-covid-19/untitled-1). Rather, it emphasizes directing patients to the appropriate level of care for their current psychiatric presentation. So what could this look like practically?
Let’s discuss how to conceptualize each bucket, resources you may be able to recommend to your patients within each, and how each might be impacted by COVID-19:
#### Self Care
Self care resources are important for maintaining day-to-day mental health and should be made available to all patients during this stressful time. Self care can come in many forms. It can include tips for stress management, advice on generating routine and setting realistic expectations during physical distancing, tools for good sleep or hygiene, and many others. Many are also turning to apps, such as Headspace and Evermind, to augment their self care, which may be appropriate to suggest to some of your patients.
For even more information, there is a handout from Massachusetts General Hospital on [Tips for Coping with the Stress of COVID-19](https://www.massgeneral.org/assets/MGH/pdf/psychiatry/HSPH-COVID-19-mental-health-tips-3-11-20_kk.pdf) and the [COVID Mental Health Initiative](https://covidstudentresponse.org/campaigns/mental-health-initiative/).
Thought Question: If you were seeing Brian in your primary care clinic, what three tools to manage stress would you first recommend?
#### Community Support
It might be challenging for patients to deal with the fear and uncertainty of COVID-19 on their own. As we have seen with Diane, many of our patients will have their existing community support greatly disrupted throughout the pandemic. Schools, workplaces, community centers, and religious organizations have all suspended their current activities. Informal community support can come through family, friends, and other organizations.
While some patients will be able to lean on friends and family to fill in the gaps lost by other social support mechanisms, others will not be able to do so. These patients may benefit greatly from connection to community resources.
Tips for talking to your patients about community resources:
* As much as possible, try to keep individuals connected to their existing community support and care organizations. For example, work to connect individuals with online versions of their recovery groups or help your patients set up streaming of their religious services;
* Do your research before recommending resources! Some community groups that you’ve worked with in the past may not be operating at this time.
#### Primary-Care Mental Health Services
If self care and community support are not sufficient, the first touch point with the health system is generally through a patient’s primary care provider. This should not change during the pandemic, although the appointments themselves may be virtual. PCPs are appropriate providers to perform mental health screening, refer interested patients to therapy, and often offer initial medical management. These core roles should not change due to COVID-19. As medical students, you may be assisting with these tasks more frequently in your primary care clinics over the next few months.
#### Psychiatric Specialist Care
The most resource-intensive mental health care is psychiatric specialist care. This includes psychiatric specialty clinics, emergency room care, and psychiatric hospital care. Given the prevalence of COVID-19 positive patients in emergency rooms, beds and personnel resources might be shifted to accommodate individuals with emergent presentations of COVID-19. Additionally, patients may not feel safe presenting to emergency rooms given their fears of contracting the infection. In the midst of these limitations, there will still be a need for providing emergency psychiatric care to patients with pre-existing mental health conditions and new patients.
In general, decisions to escalate care are complex and grounded extensively in past experience and risk assessment training. You should not be making these decisions alone. If you are worried that your patient may be unsafe in the home environment or might require inpatient or specialty psychiatric care, please consult your professor or supervisor.
*Thought Question:*
* What are three available community resources available in your area that are currently operating and that you would recommend to a patient who needed additional support?
## The Rise of Telehealth
One major change we are seeing across mental healthcare providers is an increase in telehealth utilization (for a more detailed explanation about telehealth, including practical skills about conducting an effective visit, please see Module 6). Evidence suggests that psychotherapy via teleconference shows promising results for anxiety and mood disorders ([Berryhill et al., Telemed J E Health 2018](https://www.ncbi.nlm.nih.gov/pubmed/30048211)). Despite these advantages, telemedicine has been slow to gain traction in some areas of healthcare due to policy limitations, insurance companies being reluctant to sign onto telehealth, and a slowed acceptance by healthcare professionals ([Topooco et al., Internet Interventions 2017](https://www.sciencedirect.com/science/article/pii/S2214782916300446)).
In China, as a result of the large numbers of confirmed cases and deaths, both medical staff and the public have been experiencing psychological problems ([Kang et al., Lancet Psychiatry 2020](https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366\(20\)30047-X/fulltext)). In response to this mental health crisis, online mental health education with communication companies, such as WeChat, Weibo, and TikTok, has been widely used ([Liu et al., Lancet Psychiatry 2020](https://www.thelancet.com/journals/lanpsy/article/PIIS2215-0366\(20\)30077-8/fulltext)). Throughout all 31 provinces and municipalities in mainland China, mental health professionals have established free, online psychological counselling services that are available 24 hours on all days of the week. Online psychological self-help intervention systems, including online CBT for depression, anxiety, and insomnia, have also been developed. In addition, several artificial intelligence (AI) programs have been put in use to detect potential suicidality during the pandemic.
*Thought question:*
* If a patient in Iowa has no local psychiatrists to reach out to for his mental health, would they be able to establish care with psychiatrists offering telehealth across state lines?
## Trauma-Informed Care and Universal Precautions
As the pandemic unfolds and we collectively experience this ongoing trauma as a society, our patients may feel increasingly vulnerable. This is important to keep in mind as all medical care requires a degree of vulnerability, even routine annual wellness visits. In such challenging times, we must actively seek to avoid re-traumatizing our patients.
The response to traumatic exposure may manifest in many ways. Common responses are to feel overwhelmed, unsafe, or triggered. Activation of a trauma response may manifest as a fight or flight (hyperarousal), or freeze (hypoarousal) reaction, as illustrated in the figure below. These reactions may cause an individual to move outside the “window of tolerance” within which they are able to emotionally regulate. \
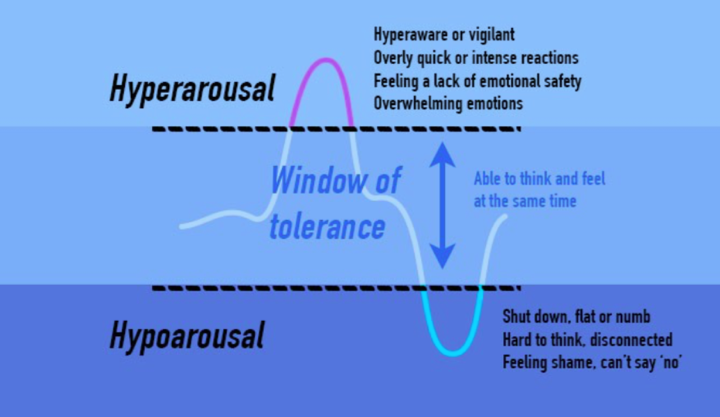
([Brickel and Associates Counseling](https://brickelandassociates.com/how-to-grow-change-after-trauma/))
It is important to recognize that everyone (providers, patients, friends, family) may experience a trauma response at any time, both during and after the pandemic. These reactions may not be linear: you may feel better one day and then worse the next. If you are feeling overwhelmed right now, some grounding techniques are included in [Module 6](https://curriculum.covidstudentresponse.org/module-6-training-for-clinical-roles/care-for-self-and-others-during-crisis) to help you through the moment; these are also useful to share with patients.
A trauma-informed care approach to patient care can actively avoid re-traumatization and also encourage our patients to develop their own strengths and resilience ([SAMHSA 2014](https://ncsacw.samhsa.gov/userfiles/files/SAMHSA_Trauma.pdf)). It is based on the six principles outlined in the figure below. As we cannot predict what clinical settings or exam maneuvers may be triggering to each individual patient, TIC should be used as a universal precaution with all patients ([Raja et al., Fam Community Health 2016)](https://www.brighamandwomens.org/assets/BWH/womens-health/connors-center/pdfs/tic-in-medicine-raja-2015.pdf). When taking a trauma-informed approach to patient care, remember that care is something you do with your patients and not something you do to your patients.
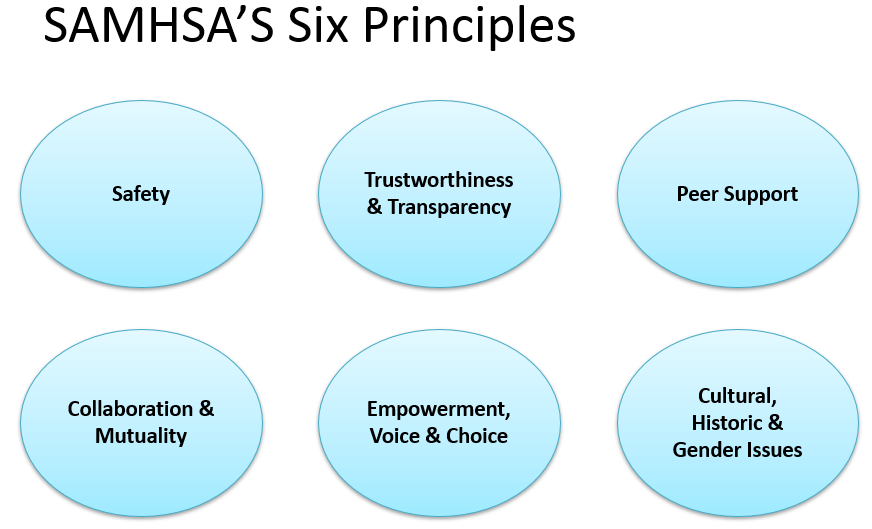
Below we’ve included some practical tips for applying the six principles of TIC to patient care. For more detailed learning, educators at Warren Alpert School of Medicine have published a course on trauma-informed physical exam ([Elisseou et al., AAMC 2019](https://www.mededportal.org/publication/10799/)). SAMHSA is another great resource ([SAMHSA 2014](https://ncsacw.samhsa.gov/userfiles/files/SAMHSA_Trauma.pdf)). Many healthcare interactions have migrated to telehealth, which warrant additional considerations for patient safety.
Here are some specific communication & physical exam tips that will help you apply the principles of trauma informed care to your future patient interactions:
1. Safety: Be aware of your physical positioning in the room, do not stand between the patient and the door, and always stay within eyesight of the patient. In a telehealth encounter, ensure the patient is somewhere they feel safe before starting the visit.
2. Trust and transparency: Offer anticipatory guidance and obtain consent for each step of the interview and before you perform any exam maneuvers.
3. Peer support: Ask the patient whether having a friend or family member present would facilitate care.
4. Empowerment, voice & choice: Reaffirm your patient’s authority to stop the exam at any time if they become uncomfortable.
5. Collaboration and mutuality: Introduce yourself and ask for the patient’s name and pronouns, and ask for and use the patient’s own terms for body parts.
6. Gender, historical, and cultural issues: Acknowledge that patients may have had negative personal or historical interactions with the healthcare system in the past, do not blame patients for their distrust of the system.