> For the complete documentation index, see [llms.txt](https://curriculum.covidstudentresponse.org/llms.txt). Markdown versions of documentation pages are available by appending `.md` to page URLs; this page is available as [Markdown](https://curriculum.covidstudentresponse.org/module-6-training-for-clinical-roles/care-for-self-and-others-during-crisis.md).
# Care for Self and Others During Crisis
## Introduction
This is a time of high risk for our patients, colleagues, families, and selves. Previously in this module we’ve discussed how to mitigate the risk of pathogen exposure; here we discuss how to mitigate the risk of traumatic exposure. Just as in previous sections, we will discuss individual actions and structural interventions that support this mitigation and celebrate the strength of healthcare workers.
**COVID-19 as traumatic exposure**
We are in a time of dramatic changes to our daily lives and reevaluation of our collective sense of safety and control. Module 5 introduced the idea that this time may represent a traumatic exposure. As caregivers, we are vulnerable both to direct effects of trauma or primary traumatization, based on our own experience of the event and secondary traumatization, in which we are affected by the suffering of those we care for. This double burden is a chronic problem for healthcare workers, and will only be magnified during the pandemic.
**How do caregivers respond to traumatic exposures?** \
\
Early studies from the COVID pandemic have already documented adverse mental health effects of COVID-19 among frontline caregivers. Experiences from China suggest high rates of depression (50.4%), anxiety (44.6%), insomnia (34.0%), and emotional distress (71.5%) ([Lai et al. JAMA 2020](https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2763229?guestAccessKey=01bafe6d-fdaa-4fb2-9401-a2ed096c1284\&utm_content=weekly_highlights\&utm_term=032820\&utm_source=silverchair\&utm_campaign=jama_network\&cmp=1\&utm_medium=email)). These effects were more pronounced in frontline healthcare workers directly engaged in triage, diagnosis, and treatment of COVID-19 patients. We share these data not to distress you, but to normalize a range of reactions that is normal for caregivers to experience during the stress of the pandemic.
Caregivers (CNAs, interpreters, nurses, providers, trainees, transport staff - everyone who touches patient care) may experience an accumulating burden of secondary trauma. In her book, [Trauma Stewardship: An Everyday Guide to Caring for Self While Caring for Others](https://traumastewardship.com/), LICSW Laura van Dernoot Lipsky lays out common elements of a trauma response. These are demonstrated in the graphic below, and animated in her [TED talk](https://www.youtube.com/watch?v=uOzDGrcvmus). You may feel several or all of these reactions.
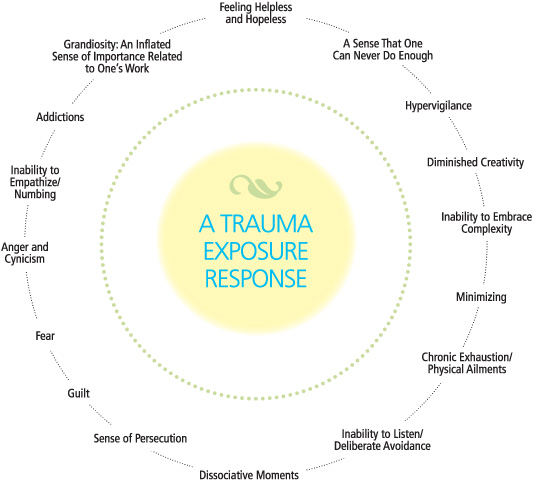
**(**[**Laura van Dernoot Lipsky, 2009**](https://traumastewardship.com/)**)**
Another common reaction to trauma, is that the reactions such as those outlined above, may feel similar to reactions you’ve had in the past, and may cause you to think about other times in which you felt overwhelmed or unsafe. You may feel triggered. You may fight, flight or freeze. These reactions refer to your “window of tolerance” within which you can emotionally regulate. Trauma exposure may cause you to fight or flight (hyperarousal) or freeze (hypoarousal). This concept is illustrated by the figure below. It is important to recognize when you might be feeling this way. We have included some grounding techniques in the next section to help get you through the moment.
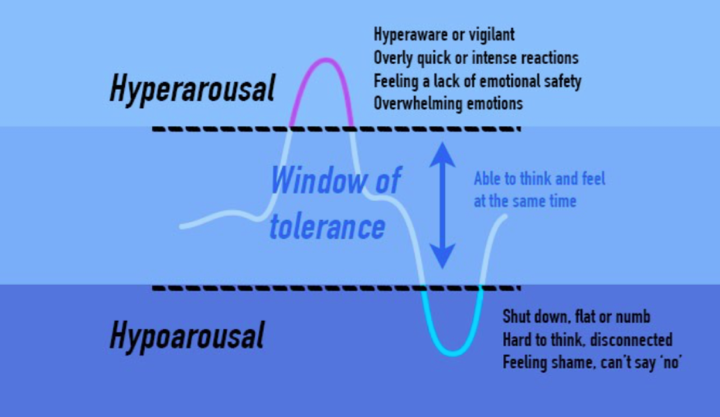
**(**[**Brickel and Associates Counseling**](https://brickelandassociates.com/how-to-grow-change-after-trauma/)**)**
Equally as important as acknowledging the losses associated with the pandemic, is highlighting the opportunities it provides for strength and growth. The figure below from the [ECHO Project](https://www.echotraining.org/trauma-trainings/) highlights 5 domains of post-traumatic growth: personal growth, closer relationships, greater appreciation for life, new possibilities, and spiritual development.
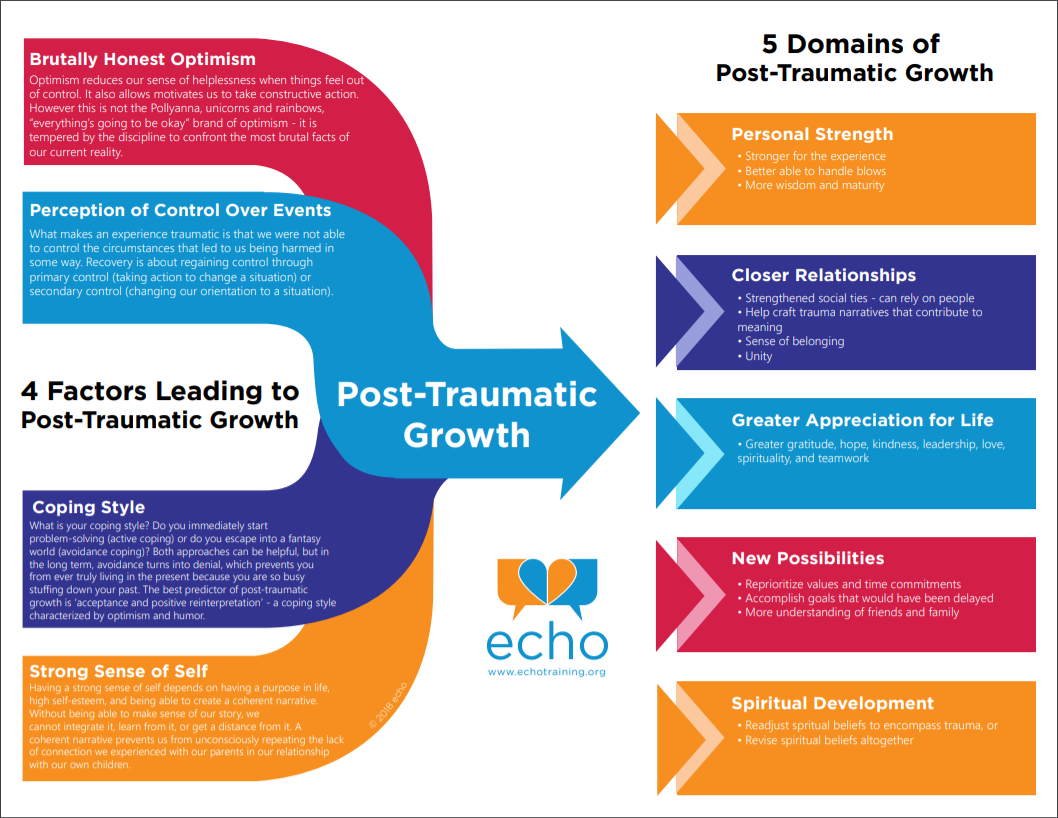
**(**[**Project ECHO**](https://www.echoparenting.org/dev/wp-content/uploads/2018/07/Post-Traumatic-Growth-Web-8x11.pdf)**)**
It is important to call out the fear and anxiety we are experiencing collectively, while also celebrating our strength as a helping profession. Even the simple act of reading through this module demonstrates your strength and commitment to staying well. By labeling the experience as traumatic, we are able to draw on the trauma-informed care (TIC) literature for guidance on how to care for ourselves.
**What can we do to mitigate the adverse impact of trauma on ourselves, our colleagues, and our patients?** \
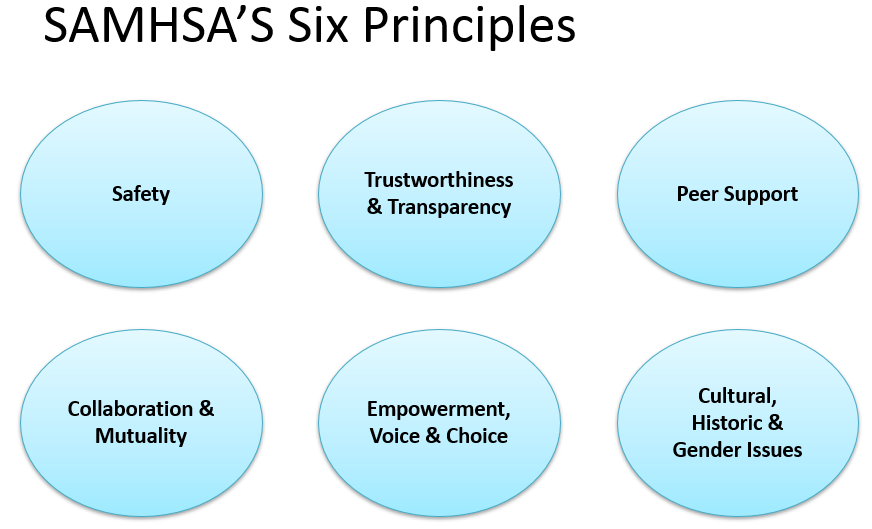
Trauma-informed care (TIC) is a strengths-based model developed to mitigate the health effects of trauma and is based on the Substance Abuse and Mental Health Services Administration’s (SAMHSA) six principles (see figure below) including: safety; trustworthiness and transparency; peer support; collaboration and mutuality; empowerment, voice, and choice; and attention to cultural, historical, and gender issues ([SAMHSA 2014](https://ncsacw.samhsa.gov/userfiles/files/SAMHSA_Trauma.pdf)). You may be familiar with trauma-informed care as a clinical model. The six principles you apply to patient care can also be used reflectively, for self-care, a practice referred to as trauma-informed self care (TISC). Here we apply the 6 principles to ourselves, our colleagues, and our institutions. The principles will be bolded throughout to highlight this framework. As you read, consider creating your own trauma-informed self care[ action plan](https://docs.google.com/document/d/1hiPP2grRxesodCOXxwfxNejopEjelSKR2Xb9s-ZJBrQ/edit).
*Thought Question:*
Think about a time you felt overwhelmed. What were some of your strengths in dealing with the situation?
### **How do we care for ourselves while performing clinical duties?**
Culturally, many healthcare providers are used to ignoring their own needs, and this is sometimes even celebrated ([Gazelle et al, 2015](https://www-ncbi-nlm-nih-gov.ezp-prod1.hul.harvard.edu/pmc/articles/PMC4371007/#CR20), [Salles and Gold, 2020](https://www.vox.com/2020/4/2/21204402/coronavirus-covid-19-doctors-nurses-health-care-workers)). However, your physical safety is critical to your psychological well-being and ability to provide care. In addition to PPE, proper meals, rest breaks throughout the day, decompression time and sufficient time off are equally as important ([Adams et al. 2020](https://jamanetwork.com/journals/jama/fullarticle/2763136), [National Center for PTSD](https://www.ptsd.va.gov/covid/COVID19ManagingStressHCW032020.pdf)). Consider high-calorie, low-volume foods such as protein bars if you anticipate you will have little time to eat during clinical care ([ACEP 2020](https://www.acep.org/corona/covid-19-field-guide/home-safety/preparing-for-work/)). Tuning in to your needs and attending to them is key to working sustainability during the pandemic.
During your clinical duties, you may notice yourself reacting to trauma such as in the reactions described above and reaching the limits of your “window of tolerance”. You might find the following framework helpful to address the emotions in the moment: Calm, Contain, Care, Cope ([Kimberg and Wheeler, 2019](https://www.springer.com/gp/book/9783030043414)).
* Calm: Do your best to remain calm in your professional environment, you may find grounding techniques particularly helpful (more below)
* Contain: Try and limit your traumatic exposure as you are able. If you are able to remove yourself from the room, do so. If a patient is disclosing traumatic events, you may remind them they do not have to share all of the details.
* Care: Be kind to yourself. Your reaction is normal.
* Cope: Reflect on positive coping strategies that have worked for you in the past- which ones are feasible in a clinical setting?
You may find grounding exercises particularly useful in the moment such as “square breathing” (inhale 4 seconds, hold 4 seconds, exhale 4 seconds, hold 4 seconds, repeat) or distraction (focus on the external environment, name all of the colors you see). More grounding techniques can be found in [SAMHSA’s Tip 57](https://www-ncbi-nlm-nih-gov.ezp-prod1.hul.harvard.edu/books/NBK207188/box/part1_ch4.box5/?report=objectonly).
You should feel empowered to advocate for your own health needs. Whether you are immunocompromised, have an underlying health condition, may be pregnant, or someone in your household has one of these conditions, you may be at higher risk for COVID complications. As a student, you do not have to act clinically if this is the right decision for your health and safety. If you do want to be involved clinically, consider lower exposure risk clinical duties, such as working from home or seeing patients virtually.
You may also find it helpful to center on the language of resilience: what allows us to bend, not break, in the face of this collective challenge? Expert clinician Nomi Levy-Carrick emphasizes three strategies for individuals and front-line health care workers alike ([Levy-Carrick 2020](https://medium.com/@ariadnelabs/the-covid-resilience-marathon-4dee79f35a51)):
1. Be able to name what is distressing in real time.
2. Insist that you should never worry alone.
3. Maintain a sense of purpose.
*Thought questions:*
What are some ways you have forgotten to prioritize your own needs in the past while working clinically?
What is one step you can take to prevent this? Consider entering it on your [action plan](https://docs.google.com/document/d/1hiPP2grRxesodCOXxwfxNejopEjelSKR2Xb9s-ZJBrQ/edit).
### **How do we care for ourselves and our loved ones at home?**
In addition to the stressors of clinical work, many healthcare workers also play an important caregiving role at home. You may worry about transmitting the virus to family or loved ones. You may face additional stressors in your home life from the disruptions caused by the virus including lack of childcare, unemployment, financial concerns, and new difficulties obtaining basic groceries and cleaning supplies. We recognize that as medical students, you may play a variety of different social roles outside of the hospital. You may be responsible for translating medical information for friends and family. Due to cultural, historical, or gender issues, you may be called on to represent a community. In this section, we will outline strategies to care for yourself and loved ones in an ongoing disaster situation.
As a first step to maintain your safety and the safety of those in your home, have a transparent conversation with your household about what to expect. What will your new clinical roles look like? How much will you be able to contribute to household activities? What will you need in terms of support? What will your household need from you in terms of support? This collaboration and anticipatory guidance can help make concrete plans for how to manage the upcoming challenges.
Consider making plans for separation of living spaces as needed to reduce the risk of transmission and home arrival routines (i.e. removing shoes and clothing, showering immediately) ([Adams et al. 2020](https://jamanetwork.com/journals/jama/fullarticle/2763136)). In addition to infection control, you may find the home arrival routine beneficial in helping you to disconnect from the clinical environment and be present in your home environment ([ACEP 2020)](https://www.acep.org/corona/covid-19-field-guide/home-safety/preparing-for-work/).
[The National Child Traumatic Stress Network](https://www.nctsn.org/sites/default/files/resources/fact-sheet/outbreak_factsheet_1.pdf) has released powerful and succinct guidelines on managing the stress of the pandemic within our household and family units. These guidelines include:
* Stay informed with media that offers transparent information while minimizing exposure to media and social media that may promote panic
* Prioritize social connection and peer support through virtual platforms such as phone calls, text, email, and video calls; or [virtual game nights](https://www.marthastewart.com/7735817/how-host-virtual-game-night) and [watching parties](https://www.netflixparty.com)
* Adhere to a consistent schedule to emphasize your choice and control, but modify to reflect current realities and limitations
* Prioritize activities that give you a sense of meaning and purpose, while still allowing yourself time to step back and take breaks as needed
* Attempt to control negative self-talk and self-defeating statements (for more information on identifying cognitive distortions and re-framing them, read [this](https://arfamiliesfirst.com/wp-content/uploads/2013/05/Cognitive-Distortions.pdf))
* Draw on your strengths; engage in activities that bring you joy and positive coping mechanisms that have worked in the past (e.g. [music](https://www.npr.org/2020/03/13/815457669/isle-of-calm-stream-6-hours-of-soothing-music), [physical activity](https://medmotion.org/covid-19-workouts/), [yoga](http://downdogapp.com/schools%20or%20downdogapp.com/healthcare))
This is a time of loss. Many trainees have lost clinical opportunities, graduation celebrations, and control of their medical education. You may have loved ones that lost a job or that have lost their lives during the pandemic. It is also a time of great uncertainty. We are not sure how long these disruptions will last and what that means for our medical training. The [National Center for PTSD](https://www.ptsd.va.gov/understand/types/disaster_help.asp) is a great resource on how to manage ongoing stress and trauma from disasters. The guidelines are similar to those above. Additionally, they emphasize reflecting positively on your losses and trying to make meaning of them either by yourself or through connection with others. For example, many of your social plans may have been canceled, but this time could allow you to reconnect with old friends or deepen existing friendships.
\
\&#xNAN;*Thought Question:*
What is one step you will take in your home life to keep yourself/loved ones well? Consider entering it on your[ action plan](https://docs.google.com/document/d/1hiPP2grRxesodCOXxwfxNejopEjelSKR2Xb9s-ZJBrQ/edit).
### **How do we care for and support our colleagues?**
For everyone, daily life has changed: first year students have been asked to leave their dormitories, clerkship students have been removed from clinical duties, healthcare workers have had to adapt to telehealth platforms or deployment to unfamiliar clinical settings overnight. Everyone is likely to have a keener sense of their own and their colleagues’ vulnerabilities. These stresses are compounded by the fact that everyone is weathering them at once. At the same time, the fact that we are all in it together enables us to offer and receive **peer support.**
**Peer support** is one of the core principles of trauma-informed care. For those who are experiencing or have experienced trauma, it can be a source of healing to connect meaningfully with others who have been in a similar situation ([Blanch et al 2012](http://www.theannainstitute.org/Andrea%20Blanch%20TIWA/EngagingWomeninTIPeerSupportGuidebook.pdf)). In this section, we define your peers as anyone who is working to support patients and their families - from those fielding triage calls to those interpreting for patients and providers; from those synthesizing [information for patients](https://covid19healthliteracyproject.com/#) to those evaluating newcomers to the ED; and from those who keep our EMRs running to those who do the critical work of [disinfecting the hospital](https://www-acpjournals-org.ezp-prod1.hul.harvard.edu/doi/10.7326/M20-2237). If you are currently in training, your peers also include trainees across your country and across the world.
Each of us who is working and learning in the context of this pandemic may switch between giving support and opening ourselves to receive it. That’s okay. When we feel up to it, what are some things we can do to support one another?
* Recognize that the ways in which people (including supervisors and teachers) respond to you may be influenced by their own trauma responses; go easy on others as you are encouraged to go easy on yourself
* When someone is feeling isolated or overwhelmed, your presence and active listening represent a source of healing. Set an intention to reach out regularly to those in your immediate environment and those who cross your mind.
* *I’ve been thinking about you and hope you’re okay. I’m happy to talk or listen or help in other ways.*
* When someone discloses an area of particular challenge, it can be helpful to express empathy, validate their experience, and offer assistance as appropriate. It is also okay to ask for this kind of support from your peers and mentors.
* *That’s so hard. I can see why you’re struggling with that. How can I help? Would you like me to help you brainstorm solutions?*
* *\[To a mentor] I am particularly worried about this person for \_\_\_ reason. What would you recommend as a next step?*
* *\[To a peer] I’m having a really hard time right now. Could we talk? / Are you in a space to help me think some things through?*
* When you are working directly with another person, being **transparent** about your limitations can **empower** both of you to fulfill your roles while respecting each other’s needs.
* *I am trained in this procedure but have never done \_\_\_ before.*
* *My housemate is high-risk; I can support virtually in any way, but not in person at this time.*
* Honor the impacts of others’ **voice and choice** with an explicit acknowledgment. One example is below.
* *\[I] just wanted to say thank you, as a fellow med student, for putting together the module… \[I] felt really validated that compassion toward patients’ and our own pasts was being incorporated explicitly.*
* **Collaboration and mutuality** come in many forms, from contributing to clinical teams in person or afar, to helping colleagues on the front lines stay afloat with childcare, groceries, and other responsibilities.
* Attend to **gender, historical, and cultural issues**. You or your colleagues may have additional responsibility as trusted sources for your communities. You or your colleagues may face an additional burden from experiencing racism or xenophobia. Acknowledge these disparities and consider what you could do as an ally.
* One primer on responding to microaggressions can be found in [Module 4](https://curriculum.covidstudentresponse.org/module-4-communicating-information-about-covid-19/cultural-humility).
*Thought question:*
* What is one action you might take to support one of your peers? (at work, at home, in community) Consider entering it on your [action plan](https://docs.google.com/document/d/1hiPP2grRxesodCOXxwfxNejopEjelSKR2Xb9s-ZJBrQ/edit).
### What can our institutions do to support us during the pandemic?
Individual and interpersonal approaches to weathering this crisis become much more effective when undergirded by institutional and structural efforts. Here we present several examples of what Boston-based medical schools and hospitals are doing to support the wellbeing of their trainees and staff, highlighting the principles of trauma-informed care.
**Medical Schools:**
* **Safety:** Pausing mandatory in-person clinical work, making virtual courses available across the full curriculum, offering clinical volunteer opportunities with safeguards to ensure students do not feel pressured
* **Trust and transparency:** Nightly Zoom calls with medical school leadership and advisors, open to the entire student body, with a centrally accessible place to submit questions and proposals
* **Peer support:** Holding digital space for written student reflections, with the option to share anonymously; organizing groups of students for weekly hang-out calls; regular student-led collective “breathing space” on Zoom
* **Empowerment, voice & choice:** Establishing faculty-mentored student task forces to allow students to act collectively in a way that is meaningful to them; one of these task forces gave rise to this curriculum
* **Collaboration and mutuality:** Faculty taking time to review student-created [educational](https://covid19healthliteracyproject.com/#) [materials](https://curriculum.covidstudentresponse.org/); faculty and staff co-authoring [articles](https://www-nejm-org.ezp-prod1.hul.harvard.edu/doi/full/10.1056/NEJMp2008006) with students; faculty and staff working to continue clinical and preclinical teaching online
* **Gender, historical, and cultural issues:** Recognizing students may have care duties within their own families and home communities, and enacting travel and attendance policies that accomodate for these duties; teaching about historical injustices laid bare by the pandemic
**Hospitals:**
* **Safety:** PPE procurement and policies - from procurement at the [national](https://www.projectn95.org/) level; to working with engineers to solve problems [locally](https://www.panfab.org/); to soliciting [donations](https://www.challiance.org/about/newsroom/personal_protective_equipment_ppe_donations_includ_1179) from the community (see [Module 5](https://curriculum.covidstudentresponse.org/module-5-training-for-medical-student-specific-roles/personal-protective-equipment) for latest institutional policies on PPE, and [Module 3](https://curriculum.covidstudentresponse.org/module-3-current-situation-and-healthcare-response/socioeconomic-ramifications#understanding-the-medical-supply-shortage) for understanding the shortages)
* **Transparency:** Daily town halls with transparent data (# COVID patients admitted, days of PPE left); dedicated internal pages maintained by hospitals to share data and the latest policies
* **Peer support:** Workers and trainees taking time to listen to one another and channel existing learning groups into peer support groups
* **Empowerment, voice, and choice:** Empowering residents to re-organize schedules to keep as many residents home and minimize back and forth to hospitals; listening to residents as they identify what they need as in-hospital support and making that happen.
* **Collaboration and mutuality:** Collaboration across specialties and professions, including “gratitude baskets” for health care workers in various roles
* **Cultural, historical, and gender issues:** Institutions need to address disparities in who is getting sickest ([Kendi, 2020](https://www.theatlantic.com/ideas/archive/2020/04/stop-looking-away-race-covid-19-victims/609250/)) and recognize that clinicians and trainees are also impacted by the world outside the hospital - that they are part of communities that may be particularly hard-hit.
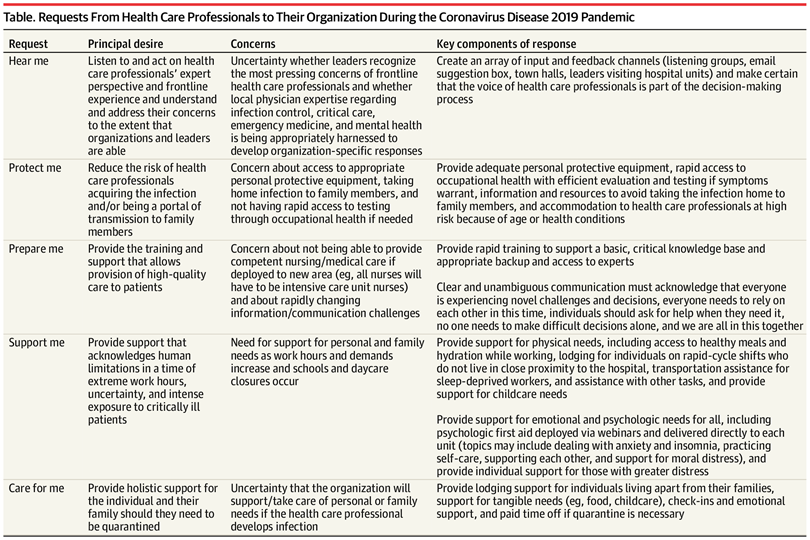
This article from [Shanafelt et al.](https://jamanetwork-com.ezp-prod1.hul.harvard.edu/journals/jama/fullarticle/2764380?guestAccessKey=01a73ac6-e78a-43e9-8ad2-6019b60b5dcb\&utm_source=silverchair\&utm_medium=email\&utm_campaign=article_alert-jama\&utm_content=olf\&utm_term=040720) (2020) collects front-line clinicians’ concerns about COVID-19 from listening sessions, exemplifying **empowerment, voice and choice**. They distill concerns into 5 “asks” from healthcare professionals to their institutions: “hear me - protect me - prepare me - support me - care for me.” Their suggestions to institutions address the need for **voice and choice** for healthcare professionals in institutional plans and **transparency** about how the situation is unfolding; attention to physical **safety; empowerment** through training for new roles; **collaboration and mutuality** across roles; and attention to the cultural issue that healthcare professionals tend to strive for self-reliance and not ask for help. Additionally they make excellent concrete suggestions for how to support health care professionals both physically and emotionally. See the full table below.
*Thought questions:*
What do you need from your institution to feel able to contribute in a sustainable way to the pandemic response? Consider noting it on your [action plan](https://docs.google.com/document/d/1hiPP2grRxesodCOXxwfxNejopEjelSKR2Xb9s-ZJBrQ/edit).
What is the role of these recommendations even in non-crisis times?
**Where can I find additional resources to stay well in close contact with trauma?**
[Self-Care When Working With Patients With Histories of Trauma](https://drive.google.com/open?id=1ZeMDwXKjSYEV_8-3W5YjcbwiQsCclXxK) (Samara Grossman, LICSW)
* [Grounding Exercises ](https://www-ncbi-nlm-nih-gov.ezp-prod1.hul.harvard.edu/books/NBK207188/box/part1_ch4.box5/?report=objectonly)
* [MGH Psychiatry Guide to Mental Health Resources for COVID-19](https://docs.google.com/document/d/11ZgNncZzNUEm24Z-Rej0g0ESGbRnd5u3cHSXTDpR5Sg/edit)
* Click [here](https://forms.gle/GaeUHAhZPGq9S2fu8) to sign up with a national network of allied health professional students.
* [Domestic Violence and Sexual Assault Resources](https://drive.google.com/open?id=1syr38-h9TEUuwCOMcB-tLvMMbReE9tVJ)
* [Safety Planning with Stay-At-Home Advisories ](https://drive.google.com/open?id=1Ax1dgWD7AISpqcm6Pq0Wg1R2dR_qtvqr)
* [Online Resources to Support Substance Use Disorder Recovery](https://drive.google.com/file/d/1VV4kgPPqCR3HLH2bPIhPL1sWaPhuGZsk/view?usp=sharing)
* Self-Service Apps: These apps, which have been clinically vetted by Partners mental health experts, are available and offer a range of support.
* [The Headspace app](https://www.headspace.com/headspace-meditation-app), available via iOS, Android or desktop, offers sets of guided meditations aimed at tackling problems related to anxiety, sleeplessness and relationships.
* [The Evermind app](https://apps.apple.com/us/app/evermind/id1485424497), available via iOS and Android, can help you build resilience and handle stress using cognitive behavioral therapy techniques. In the app, you can access guided programs on improving sleep, disconnecting, challenging negative thought patterns and more.